Contact Us
We invite you to learn more about our program and how we can care for you and your unborn baby. Please contact us at 401-228-0559 or via e-mail at [email protected].
Congenital lung lesions occur when a portion of lung tissue develops abnormally during otherwise normal fetal development. We don’t know why they form, but the ways they differ from each other may have to do with the timing and location of their development.
We invite you to learn more about our program and how we can care for you and your unborn baby. Please contact us at 401-228-0559 or via e-mail at [email protected].
There are four broad categories of lesions:
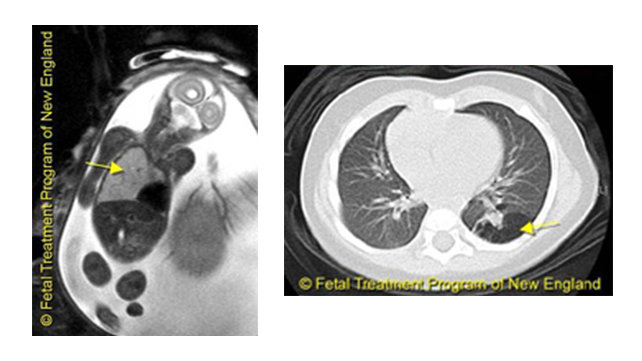
Left: Congenital lobar emphysema: overinflated right lung pushes the heart to the other side.
Right: CCAM on a CT scan after birth.
How common are they?
Congenital lung lesions are seen in approximately one in 3,000 births. They are most often isolated findings with no association with chromosomal or genetic disorders. CCAMs and sequestrations are sometimes seen in fetuses with congenital diaphragmatic hernia; however, many are discovered by chance in otherwise healthy children or children with unrelated anomalies.
How are they diagnosed?
Before birth, they are diagnosed through ultrasound and fetal magnetic resonance imaging (MRI). They can also be discovered accidentally, on a chest x-ray, later in childhood or even adulthood.
What can happen before birth?
Lesions are not usually visible until early in the second trimester. By the middle of the second trimester, they can be quite large. Most become smaller without causing permanent damage, in which case there is no reason to intervene before birth. However, they should be monitored with weekly ultrasounds or a fetal MRI until it is clear that the lesions are getting smaller. If the lesions grow too fast, one or both lungs may become compressed. The heart may be pushed to one side and compressed, which can lead to heart failure.
What can be done before birth?
If the lesion grows and there are signs of heart failure after 25-26 weeks of pregnancy, early delivery is usually recommended. If these signs occur earlier in pregnancy, delivery is not an option because the baby can’t survive outside the womb. Intervention on the fetus can be risky but is usually possible through:
What are my delivery options?
Unless there are signs that the fetus is in trouble, pre-term delivery or Cesarean section is not necessary. Cesarean section may be necessary for obstetrical reasons, however. It is recommended that mothers deliver in a hospital that has immediate access to a specialized neonatal intensive care unit (NICU), with a pediatric surgical specialist present. In some cases, the lesion is so large at birth that immediate surgical intervention is needed.
What will happen at birth?
Neonatologists will be present to assess the baby and start treatment if necessary. In most cases, the mother can see and hold her baby after delivery. Afterward, the baby will go to the NICU to make sure he or she is breathing easily.
If there are no complications, the baby will undergo imaging tests, such as a chest x-ray or ultrasound, to examine the lesion. Babies who breathe well and show no other signs of distress do not need immediate intervention and may go home within a few days. However, it is important to schedule a consultation with a pediatric surgeon before leaving the hospital. Surgical intervention is often recommended later in infancy, typically between six and 18 months.
If the baby has breathing difficulties due to the lesion, an operation may be needed sooner—sometimes immediately after birth. Part of the lung may be removed through thoracoscopy (“keyhole” surgery) or open surgery. The procedure is very safe and nearly all babies recover fully. The remaining lungs will continue their normal growth.
What is the long-term outcome?
The overall outcome is generally good if the lesion has shrunk by the time of birth. CCAMs are at a significant risk of recurrent infections like pneumonia; however, this can be avoided by removing the lesion. It is recommended that all lesions be removed in early childhood to avoid risks later on.